How Long Will Olfactory Dysfunction Last Following COVID-19 Infection? How To Remove Long COVID loss of smell?
- Long Covid Classified Treatment Options
- 08 Nov, 2022
Summary
Numerous studies have confirmed that novel coronavirus infection in humans produced long-lasting side effects even after the symptoms of the initial infection disappeared completely, which we call long-term COVID symptoms. These effects of post-coronavirus remnants mainly were the appearance of brain fog, fatigue, shortness of breath, chronic pain, loss of smell, loss of taste, and diarrhea. These post COVID symptoms can put eternal side effects on the body.
According to published medical research papers, long-term COVID-19 symptoms are mainly caused by the damage to the body's own immune system and inflammation following COVID-19 infection. Studies have also shown that for a small proportion of patients with COVID-19, as trace amounts of coronaviruses remain latent in their bodies for a long time, this residual trace amount of live virus will continue to invade the body's cells and repeatedly activate the immune system, leading to long-term inflammatory response. This long-term effect is concentrated in the heart, kidneys, and brain, in addition to being manifested in the lungs.
In this paper, the author studied the long-term COVID-19 syndromes,finding that loss of smell was more frequent and the pathogenesis was more complex, so the post COVID syndrome of loss of smell was particularly studied.This paper summarized the characteristics of COVID-19 syndrome of chronic loss of smell and gave in-house self assessment to judge whether people develop these symptoms of loss of smell. Then,the pathogenesis of olfactory dysfunction caused by long-term COVID-19 was analyzed, and the therapeutic ideas of western medicine for olfactory dysfunction after infection with COVID-19 were given.
Due to the limitation of western medicine treatment against long-term COVID loss of smell, this paper also recommended some traditional Chinese medicine, including Chinese medicine formula and acupuncture treatment, to treat the related symptoms of loss of smell. In addition, this paper made advises patients with long COVID loss of smell on taking health care products, as well as on exercise, diet, and sleep. In the end, we hope that the treatment program for long-term COVID loss of smell suggested in this paper could benefit patients by improving their symptoms of discomfort of smell as soon as possible, and even cure the loss of smell caused by novel coronavirus.
Keywords: Long COVID, Post COVID-19 Symptoms, Long COVID loss of smell, Post COVID-19 Symptoms of loss of smell, long-term COVID-19 symptoms of olfactory dysfunction, post long COVID symptoms of loss of smell.
1.What Are The Manifestations Of Long-Term COVID-19 Olfactory Dysfunction?
Since the COVID-19 pandemic, after being infected with these coronaviruses, some people experienced olfactory dysfunction, such as the loss of smell or olfactory disorder.Sometimes the loss of smell is continuous and sometimes intermittent, usually lasting for a long time, even up to more than a year. This condition is called long COVID olfactory dysfunction. According to statistics in the study report, approximately 10% of people infected with novel coronavirus developed long-term COVID, and patients with loss of smell accounted for one-fourth of all patients with long-term COVID. That means about 2.5% of people infected with the coronavirus would experience loss of smell. According to published medical papers on long COVID symptoms of olfactory dysfunction, we conclude that the manifestations of loss of smell are as follows:
(1)Loss of Smell: Smell dysfunction, feel that the nose does not smell, or smell abnormality.
(2)Associated symptoms, Alzheimer disease: a neurodegenerative disease that occurs frequently in old age and is also called senile dementia. It is characterized by generalized dementia such as memory impairment, aphasia, visuospatial skill impairment, and executive dysfunction.
(3)Potential associated symptom, Loss of Taste: taste dysfunction, feel that the tongue does not taste, or taste abnormality.
(4)Potential associated symptom,Blurry vision: it is easy to experience blurry vision and dry eyes when reading articles on computer screens and mobile phone screens and feel fatigued when recognizing things through eyes; feel that eyes are pain caused by the sunshine, and when exposed to sunlight, one feels easily dizzy; feel eyeball fatigue when being close to looking at the smaller font of text or small details.
(5)Potential associated symptom,Chronic headache: feel chronic headache throughout the whole brain, or symmetrical chronic headache bilaterally in the brain; frequent feel of fever and tightness in the head. Some presented with tension headaches or migraines.
(6)Potential associated symptom,Sleep disorder: difficulty in falling asleep,easy to wake up, poor sleep quality, or feel drowsiness and it is difficult to wake up.The patient presented with the conditions of day and night reversal, staying up late, and feeling tired in the daytime and energetic at night.
2.How Long Will Olfactory Dysfunction Last After Being Infected With COVID-19?
2.1 What is Long COVID?
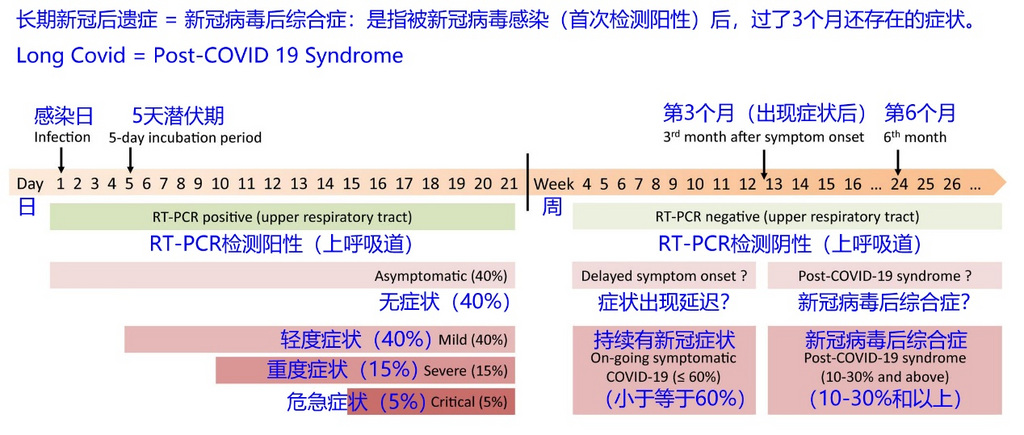
According to the definition of the World Health Organization, Post-COVID Conditions or Long COVID, also known as Post COVID-19 syndrome, refers to since the patient was infected with the novel coronavirus, the results of his PCR showed positive as criteria, and he still suffers uncomfortable symptoms after 3 months. More detailed updated statistical information on the incidence of Post COVID-19 Symptoms according to the timeline can be found in the figure below.
Post COVID-19 Symptoms are mainly concentrated in five aspects, including respiratory syndrome, cognitive system syndrome, chronic fatigue syndrome, chronic pain syndrome, and mental syndrome, such as long COVID brain fog, which belongs to the cognitive system syndrome. Long COVID chronic fatigue are one of chronic fatigue syndrome. According to medical classification, cognitive system syndrome includes fatigue symptoms, chronic fatigue syndrome, and brain fog. Moreover, two symptoms such as brain fog and loss of smell will coexist in many patients with long COVID.
If you have been infected with the novel coronavirus before, which means your previous result of PCR test showed positive, and before infection with the novel coronavirus, you didn’t suffer from the long COVID symptoms of loss of smell, but now you are presenting these symptoms of loss of smell in the above section, you are likely to afflict by long COVID-19 symptoms of loss of smell.
2.2 How Long Will Symptoms Of Loss Of Smell Last Following COVID-19 Infection?
How long will COVID-19 loss of smell last? Olfactory Dysfunction caused by COVID-19 infection usually last 10 to 14 days. But even after recovery from acute symptoms early in COVID-19 infections, people still feel Olfactory Dysfunction. A study found that more than half of people still experience Olfactory Dysfunction for up to six months after illness.
In 2021, in a study designed to describe long-term COVID-19 symptoms in more than 3,000 people from 56 countries, researchers found that 88% of respondents represented brain fog symptoms such as cognitive, headaches, Olfactory Dysfunction and memory problems. During the first few months after the onset of COVID-19 symptoms, these symptoms showed an increasing trend and then started to decrease gradually. At the beginning of the 7th month after the onset of COVID-19 symptoms, 55.5% of respondents reported suffering from cognitive problems such as brain fog.
A 2022 study investigated the rehabilitation of individuals with neurological symptoms such as long-term COVID-19 brain fog. The mean duration of brain fog since participants developed symptoms of COVID-19 infection was 14.8 months. After an initial evaluation, participants were followed up for 6 to 9 months. During follow-up, no significant changes were observed in the reporting of brain fog symptoms compared with the initial assessment, which means there was no significant change among most patients with brain fog. Researchers still pointed out that the quality of life measures of study participants remained lower than that of the general population.
According to published medical statistics papers on long-term COVID brain fog, the symptoms could last for quite a long time. The symptoms of brain fog tend to peak within a few months of infection with COVID-19 and then generally begin to improve over time. However, brain fog may still persist for several months. Recent studies have found that brain fog symptoms may last more than a year after infection with COVID-19. Moreover, studies have shown that more than 20% of patients with long-term COVID brain fog still did not get an improvement for their symptoms after a year.
3.What Are The Causes Of The Chronic Loss Of Smell After The COVID-19 Infection?
3.1 Why Can Humans Smell? What Is The Principles Of Human Olfaction?
Before answering this question, let’s begin to understand the principles of human olfaction, which is why humans can smell odors.
(1) Odors are transmitted in the air, so when humans inhale air from the outside through the nasal cavity, or exhale air from the lungs through the nasal cavity, odor molecules in the air pass through the nasal cavity.
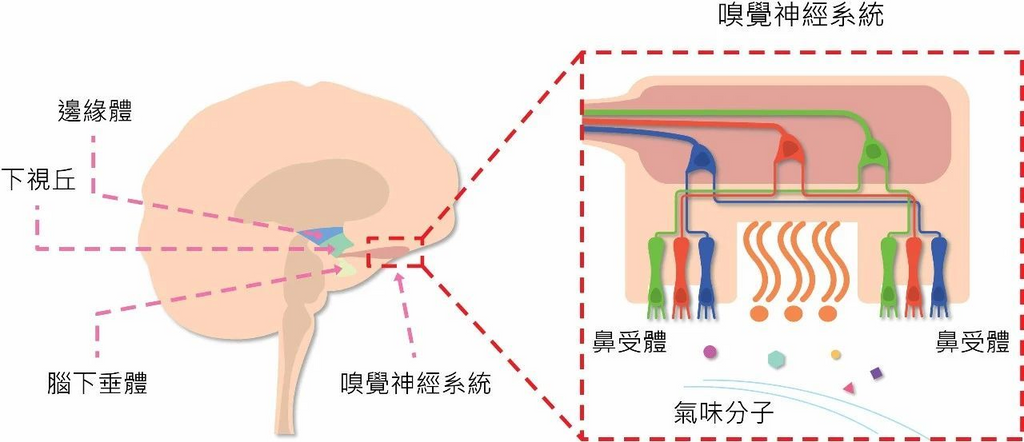
(2) There is a region on the top of the nasal cavity called the olfactory epithelium, which is the olfactory nervous system. Olfactory epithelium contains olfactory neuron cells and olfactory epithelial sustentacular cells. Sustentacular cells of the olfactory epithelium are designed to protect and support olfactory neuronal cells in order to function normally.
(3) Above the olfactory epithelium, there is a bone with many dense holes, which we call the ethmoid bone. There is also a tissue above the ethmoid bone, which we call the olfactory bulb. Olfactory neuron cells pass through many dense holes in the ethmoid bone and connect the olfactory epithelium and the olfactory bulb.
(4) Abundant cilia will form in the lower part of olfactory neuron cells, and various GPCR proteins that can capture various odorant molecules will be distributed on the cilia. The structure of this protein can chime with the structure of odorant molecules. When an odorant molecule passes through the olfactory epithelium, it is captured by various GPCR proteins through a chimeric effect.
(5) The GPCR protein then detaches from the olfactory neuron along with the chimeric captured odorant molecules, and while detaching, the cilia of the olfactory neuron cell release neuroelectric signals, which are instantaneously transmitted to the olfactory bulb.
(6) Inside the olfactory bulb, the other side of the olfactory neuron cell is connected to the mitral neuron cell. The neuroelectric signal is then transmitted to mitral neurons, which then travel to the olfactory brain in the brain.
(7) Olfactory brain in the brain, by decoding the electrical signals transmitted by mitral nerve cells, and then matching cognition and memory, can determine what kind of odor this thing emits.
Human olfaction is important, and the olfactory nervous system of humans directly links the olfactory brain parts of the brain and reaches the limbic system of the human brain. Olfaction and human memory are deeply intrinsically related, and this key lies in the olfactory brain. The olfactory brain is located in the limbic system and processes odors, emotions, and memories, also known as the emotional brain and memory brain, which can directly reflect the human psychological state, stimulate emotions, and evoke a certain memory.
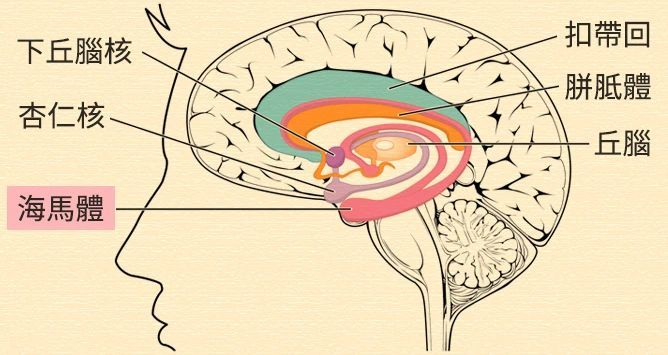
Components of the limbic system include the hippocampal gyrus, parahippocampal gyrus and entorhinal region, dentate gyrus, cingulate gyrus, mammillary body, and amygdala. Among them, the amygdala directly responds to external stress and processes direct and primitive emotions such as fear and anger. The hippocampus processes basic learning, spatial or sixth sense and is associated with memory. The cingulate gyrus processes emotions in the limbic system and is also connected to the cerebral cortex and is associated with rational, profound creative, and learning power.
Thus, any odorant molecule that reaches our limbic system initiates three responses: odor, emotion, and memory. Therefore, when we smell a specific odor, it will be accompanied by the memory, which is the plot that occurs when the specific state at that time, causing deep memory and response. Regardless of pleasant, horrible or tragic memory, all will be accompanied by physiological reactions, together stored in the limbic system. Odors are not divided into good and bad, and what distinguishes is that odors bring us emotions and memories, and everyone has different feelings about tastes due to their different experiences. Once humans lose their sense of smell, it is not just the problem of not being able to smell, but the emergence of various odor-related cognitive impairments, even putting humans at great risk. For example, if gas leakage occurs, people with loss of smell can not smell the gas in the air, it is easy to produce gas poisoning or fire.
According to the rationale for humans can smell in the above paragraphs, and the published medical papers on chronic loss of smell in long-term COVID, we conclude that there are three conditions in the pathogenesis of chronic loss of smell after long COVID-19:
(1) In patients infected with novel coronavirus, the virus invades olfactory epithelial Sertoli cells through the ACE2 receptor and triggers inflammation and pyroptosis of olfactory epithelial Sertoli cells. In turn, it destroys the nutritional and environmental support of olfactory epithelial Sertoli cells to olfactory neuronal cells, resulting in abnormal function, inflammation, and even death of olfactory neuronal cells. When olfactory neuron cells function abnormally, GPCR proteins cannot be made to chimerize to capture odor molecules, and at this time, people cannot smell odors. This is one of the causes of loss of smell or olfactory abnormalities.
(2) In patients infected with novel coronavirus, if the virus further invades epithelial cells in the olfactory bulb, such as capillary epithelial cells, it triggers inflammation of the olfactory bulb or even atrophy of the olfactory bulb, which disrupts the transmission of electrical signals between olfactory neuron cells and mitral neuron cells. At this time, people can not smell. This is also one of the causes of loss of smell or olfactory abnormalities.
(3) Patients infected with novel coronavirus infection, if the virus further invades the olfactory brain, that is, the part of the limbic system of the brain responsible for the processing of olfactory electrical signal coding and decoding logic operations. This makes the electrical signals of the olfactory nervous system hard to be understood and operated normally by the brain, which is one of the causes of loss of smell or olfactory abnormalities.
3.2 The Process Of Novel Coronavirus Invading The Brain Through The Olfactory Nervous System And Leading To Olfactory Dysfunction
Studies have shown that patients infected with COVID-19 can trigger inflammation of the olfactory bulb or even atrophy of the olfactory bulb if the virus further invades epithelial cells in the olfactory bulb, such as capillary epithelial cells, which disrupts the transmission of electrical signals between olfactory neuron cells and mitral neuron cells. Based on the above studies, we can deduce the process of how novel coronavirus invades the brain through the olfactory nervous system. If the virus further invades the olfactory brain, which is the part of the limbic system of the brain that is responsible for the processing of logic operations for the encoding and decoding of olfactory electrical signals, this makes the electrical signals of the olfactory nervous system unable to be normally understood and operated by the brain, which is the cause of cognitive dysfunction.
The following figure shows how the novel coronavirus invades the brain through the olfactory nervous system and leads to brain inflammation:
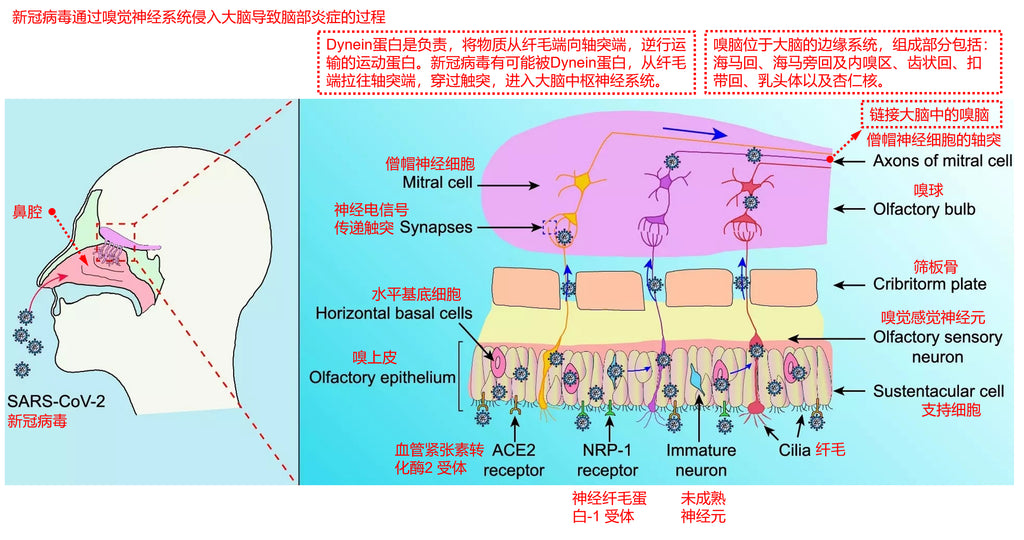
(1) Novel coronavirus enters through the respiratory tract and attaches to epithelial cells of the upper respiratory tract and lungs. The novel coronavirus recognizes host receptors via the spike glycoprotein (S protein) of coronavirus.
(2) It then binds to ACE2 (angiotensin-converting enzyme 2) receptor and TMPRSS2 (transmembrane serine protease 2) receptor and enters Sertoli cells of the olfactory epithelium and horizontal base cells of the olfactory epithelium in a membrane-fused manner.
(3) Extracellular vesicles (EV) are nanoscale membrane vesicles composed of lipid bilayers and secreted by all cell types. They act as carriers, protecting macromolecules such as proteins and RNAs from enzymatic degradation, and transporting these macromolecules between different cells, from adjacent cells to more distant cells, or immune cells. In addition, specific extracellular vesicles (EVs) have been shown to be able to cross the brain barrier.
(4) Very small amounts of novel coronavirus in Sertoli cells of the olfactory epithelium and horizontal base cells of the olfactory epithelium may be encapsulated into extracellular vesicles (EVs) and then enter olfactory neuronal cells.
(5) In neuronal cells, Dynein protein is the motor protein responsible for retrograde transport of substances from the cilia end to the axons end. The novel coronavirus is likely to be pulled from the cilia end of olfactory neurons to the axonal end by the Dynein protein, thereby entering the olfactory bulb.
(6) In the olfactory bulb, olfactory neurons and mitral neurons communicate neuroelectrical signals through touch process connections, at which time novel coronavirus may be encapsulated into extracellular vesicles (EVs) and then into mitral neuron cells.
(7) In mitral neurons, novel coronavirus may be retrogradely transported by Dynein protein into deeper brain neurons and thus enter the central nervous system of the brain.
From published medical research papers, most studies agree that COVID-19 patients develop extensive inflammation of the olfactory mucosa and bulb. (Emmi et al, 2021; Matschke et al, 2020; Meinhardt et al, 2021; Schwabenland et al, 2021; Thakur et al, 2021). Douaud et al investigated structural brain changes before and after SARS-CoV-2 infection in a large sample of British Biobank participants, revealing significant reductions in gray matter thickness and tissue contrast in the orbitofrontal cortex and parahippocampal gyrus, as well as significant functional changes in brain regions connected to the primary olfactory cortex.
Inefficient metabolism of the olfactory brain, including the olfactory gyrus and contiguous limbic/paralimbic regions, extending to the brainstem and cerebellum (Guedj et al., 2021), and right parahippocampal gyrus and right thalamus (Sollini et al., 2021) has also been reported in images obtained from positron emission tomography (PET) brains of patients with Long COVID-19 patients.
Regarding neuroinflammation occurring in the olfactory system of COVID-19 patients, Schwabenland et al. (2021) performed a deep spatial analysis of local immune responses by imaging mass spectrometers, revealing significant immune activation in the medulla oblongata and olfactory bulb, in which CD8 + T cells-microglia, crosstalk in the parenchyma mediated a significant effect. Similarly, other authors (Emmi et al., 2021; Matschke et al., 2020; Solomon et al., 2020) detected significant astrogliosis, microglial activation, and microglial nodules in the brainstem and olfactory structures of COVID-19 subjects. These are evidence of brain inflammation.
There is also a situation that there are trace viruses that escaped in the human body in the long term, which will persistently infect and invade human tissue cells, causing tissue damage. Tissue damage, in turn, triggers chronic inflammation. This chronic inflammation is produced by a persistent immune response, also causing persistent massive cytokine diffusion.The continuous breakdown of a large number of cytokine proteins can lead to autoimmunity. Autoimmunity refers to the immune response produced by organisms against healthy cells and tissues of their bodies. Any disease caused by this immune abnormality is called autoimmune disease.
The persistence of trace novel coronavirus continues to deteriorate the situation, leading to T cell failure and immune memory defects. Defects in immune memory can make the immune system gradually insensitive to immune pathways that eliminate novel coronavirus, eventually becoming a coexisting state. This condition is characterized by generalized diffuse chronic inflammation. It has been confirmed that certain markers of proinflammatory responses, which also break through the blood-brain barrier under stress, invade the brain and trigger neuroinflammation and neurodegenerative diseases. This condition can further cause metabolic abnormalities in the brain, such as cerebral capillary microthrombi, local nerve cell hypoxia in the brain, and so on, which may also be one of the causes of long-term coronary symptoms of loss of smell.
4.How To Treat The Long-Term COVID-19 Symptoms Of Loss Of Smell?
At first, we need to take a thorough physical examination of our bodies, and besides taking routine examinations, we need to do another four examinations.
The first item: do several more PCR tests, and nasal and throat secretions should be dipped enough to check whether the result shows positive. If it shows positive, it means there is still some active novel coronavirus in the body.
The second item: perform a specific examination according to the pathogenesis of loss of smell. Endoscopic examination of the nasal cavity, especially the olfactory epithelium, is performed first for lesions, such as symptoms of redness and inflammation. A standard olfactory test shall be also performed to assess the degree of olfactory impairment.In order to avoid ignoring potential risks, further examine whether the olfactory bulb, olfactory brain, and limbic regions of the brain are abnormal by CT scanning.
Because hyposmia is also a well-known early symptom of Parkinson's disease, following unconventional deeper neurological tests can be performed. For example, to rule out testicular brain injury, physicians are advised to perform functional magnetic resonance imaging MRI of the brain, including functional magnetic resonance imaging MR angiography of the brain. In elderly patients, imaging findings of early abnormal brain changes in Parkinson 's disease, Alzheimer' s disease, or other types of neurodegenerative dementia can be excluded by functional magnetic resonance imaging MRI of the brain.
When patients report memory impairment, it is important to determine whether this memory impairment is caused by infection with COVID-19 or whether COVID-19 infection worsens pre-existing symptoms. If ischemic or hemorrhagic stroke is observed on functional magnetic resonance imaging MRI of brain, we must consider medical therapy to prevent recurrent stroke.
Perfusion imaging (single photon emission computed tomography) may also be performed if the patient is wealthy or if the physician suspects the diagnosis. Cerebral perfusion imaging, which is perfusion imaging using CTP and MRP, has become a routine method to examine cerebral blood flow perfusion in stroke patients. Although there is still no evidence that perfusion imaging is an essential test for stroke assessment, many centers have begun to use perfusion imaging to assess cerebral blood flow in patients.
Cerebral perfusion testing may also show the inflammation triggered by non-specific immunity (innate immunity, which refers to the normal physiological defense function congenitally possessed by the body and can make the corresponding immune response to the invasion of various pathogenic microorganisms and foreign bodies) , which is characterized by hypoperfusion in the prefrontal or temporal lobes. Although there is no established treatment for this problem, some drugs that develop brain blood may help improve the condition.
Third item: in addition to basic blood tests, we assessed thyroid hormones, zinc, ferritin, antinuclear antibodies, rheumatoid factor, and blood sedimentation rate in almost all patients. Patients with PASC may have electrolyte disturbances, anemia, thrombocytopenia, hypoalbuminemia, lipid abnormalities, and abnormal glucose metabolism. These data need to be combined with patient symptom descriptions to carefully analyze the pathogenesis behind reasoning to determine whether abnormal laboratory test results can explain the symptoms of PASC.
The fourth item: listen to the sounds of the heart and respiratory system with a stethoscope. Anemia, the signs of heart failure, latent arrhythmias such as atrial fibrillation, and pneumonitis from enteritis must be assessed when abnormal sounds are detected, or if breathlessness persists, and to check whether oxygen saturation decreases during exercise.
The following items, from item 5 to item 7, are required when the patient presents other symptoms.
Fifth item: rheumatoid arthritis or other related diseases must be analyzed when patients have symptoms of joint discomfort.
Sixth item: when the patient complains hair loss, we examine the scalp, return to the history of hair loss symptoms, and confirm the weekly amount of hair loss.
Seventh item: neuropsychological tests should also be performed if the patient has significant psychological problems.
Then, the results of the above comprehensive physical examination and four special examinations should be handed over to the doctor, and then the person should communicate with the doctor to describe one’s own long-term COVID symptoms of loss of smell in detail to him.
Additionally, the doctor can design the best treatment for you. Because the situation varied from person to person, after the interview the treatment plan given by the doctor is also different, so this paper cannot give a general treatment plan.
The rough ideas for designing the treatment plan are as follows:
(1) According to the results of the patient's comprehensive physical examination and four special examinations as well as the communication with the patient, find out the most likely pathogenesis of the patient's long-term COVID symptoms of loss of smell, namely exploring the reason.
(2) Prescriptions are prescribed for treatment according to the pathogenesis and the patient's physical condition.In most cases, the ofactory nervous system is found to be in a state of chronic inflammation, and at this time, treatments against neuroinflammation are usually used.
(3) For the main direction of medication, if novel coronavirus remains in the body, antiviral drugs such as Paxlovid should be used as a priority. If there is no virus in the body, the drug is used from the perspective of reducing or eliminating the chronic inflammation of the patient, improving the metabolic circulation and immune mystery of patients. For example, rintatolimod (immunomodulator) and coenzyme Q10 + NADH (mitochondrial modulator) can be used to improve the immune system of patients,.
(4) The olfactory nervous system shall be immediately trained for olfactory recovery under the guidance of a physician.Generally, olfactory recovery training consists of three parts: odor essential oil, corresponding image card of cognitive recognition, and nasal wash. The common essential oils used are sweet orange essential oil, eucalyptus essential oil, rose essential oil, lemon essential oil, and clove essential oil. Recognition cards of cognitive image are images with text, and memory points corresponding to different essential oils, accompanied by olfactory conduction diagrams. Nasal wash can be usually performed with normal saline or normal saline supplemented with trace amounts of corticosteroids. Adherence to olfactory recovery training will achieve good results with twice a day, 1 minute each time for three months .
(5) Massage of the nasal cavity may also be tried as studies have shown that this is also beneficial for olfactory recovery.
5.How To Treat Long COVID-19 Symptoms Of Loss Of Smell From a Traditional Chinese Medicine(TCM) Perspective?
From the theory of syndrome differentiation and treatment of TCM, the treatment of long-term COVID symptoms of chronic loss of smell can obtain more accurate TCM syndrome differentiation and more suitable TCM formulas from the following three steps.
(1) Perform the observation, smelling, hearing, and inquiring of traditional Chinese medicine diagnosis, and consult the comprehensive physical examination report and four special examination reports of western medicine in the previous section at the same time. Only in this way can TCM doctors obtain the most detailed disease information of patients to support them to make the most accurate syndrome differentiation and treatment of patients' conditions.
(2) TCM doctors will classify and summarize the main symptoms, accompanying secondary symptoms, physical condition, and sick parts of the internal organs of the patients according to the most comprehensive disease information of the patients. First, the main symptoms are the most unbearable symptoms of patients at present, such as loss of smell. Second, accompanying secondary symptoms are that suffered from the main symptoms, which means the patient is experiencing other uncomfortable symptoms, such as mental turbidity, chronic headache and so on. Third, to find out the physical condition of the patient, which means the patient's current physical health status, belongs to which category in the TCM constitution. For example, yang-deficiency constitution, phlegm-dampness constitution, qi-deficiency constitution, blood stasis constitution, etc.
(3) TCM doctors, according to the above summary, combined with the internal organs and meridians related to symptoms, comprehensively use the theory and practical experience of TCM to make TCM prescriptions for patients.If acupuncture and moxibustion are required, these programs will also be prescribed.
Traditional Chinese medicine (TCM) theory is mainly based on: Zhang Zhongjing’s “Treatise on Febrile Diseases”, “Synopsis of Golden Chamber”, Huang Yuanyu's “Four Sacred Hearts Source”, “Typhoid Fever Suspension”, “Jinkui Suspension”, “Changsha Yao Jie”, Li Dongyuan 's “Treatise on the Spleen & Stomach”, and Zhang Jingyue' s “Jingyue Quanshu”.
TCM Practical experience, which can be found in Google Scholar (Fig. https://scholar.google.com/), and search for keywords for TCM treatment of long-term novel coronavirus symptoms. For example, COVID-19 Traditional Chinese Medicine, Long COVID Traditional Chinese Medicine. A large number of academic papers on medical research on the treatment of Long COVID by traditional Chinese medicine can be found in this way.
In order to make it easier for everyone to understand the treatment process of TCM, the following is a TCM treatment case of a patient with long-term COVID-19 symptoms of loss of smell.
Case 1:
Name: Yang, female, aged 47 years, height 155cm, weight 60 kg.
MEDICAL HISTORY: PCR was positive for novel coronavirus on 26 August 2022, followed by typical symptoms of novel coronavirus infection: fever, cough, sore throat, sputum with blood streaks,anosmia and loss of taste. Two weeks later, the symptoms of novel coronavirus infection gradually relieved and disappeared. Later, long-term COVID symptoms of loss of smell and olfactory dysfunction appeared successively.
Physical examination report of western medicine: (1) PCR test for novel coronavirus showed positive results again.(2)The olfactory epithelium area, showing symptoms of redness and inflammation. (3) Proinflammatory markers were high and there was slight systemic chronic inflammation. (4) Immune system examination items revealed abnormal lymphocyte subset determination, C-reactive protein, and immunoglobulin data.
Main symptoms: loss of smell, throat itching.
Accompanying secondary symptoms: occasional mental turbidity and chronic headache.
Prescriptions given by Western physicians:
(1) Paxlovid (paxlovid, antiviral drug, use to prevent the replication of novel coronavirus in vivo).
(2) Coenzyme Q10 + NADH (mitochondrial modulator).
(3) Rintatolimod (immunomodulator).
(4) Vitamin C, vitamin E, sulforaphane and resveratrol. (Use to reduce the inflammatory reaction in vivo.)
TCM constitution: the body presents phlegm-dampness constitution.
TCM diagnosis evaluation: nasal deafness caused by exogenous wind pathogens, wind-heat in the lung meridian, and slight deficiency of both lung and spleen, resulting in loss of smell and abnormal olfaction.
Prescription given by the TCM doctor:
(1)Danggui Shaoyao Powder plus fried Xanthium sibiricum is used to clear away heat and toxic substances, eliminate olfactory nervous system inflammation, and reduce olfactory loss symptoms.
(2) Mailuotong capsule is used to dredge meridian vascular congestion.
(3) Lanqin Oral Liquid is used to improve sore throat and itchy throat.
Acupuncture program given by the TCM: electricity is exerted to heat the moxibustion apparatus, and apply moxibustion at the following acupoints.
(1)Yingxiang, Baihui and danzhong points are used to improve upper respiratory tract inflammation and promote metabolism.
6.Which Kind Of Health Products Are Beneficial To Improving Long-Term COVID Symptoms Of Loss Of Smell?
Taking the patient above as an example, we give the following health product recommendations based on her condition:
(1) Omega 3 (Ω3) fatty acids, containing high amounts of DHA and EPA, are used to improve fatigue function and protect against cardiovascular and cerebrovascular diseases.
(2) VC,VD and VE are used to scavenge free radicals, anti-oxidation, and reduce systemic chronic inflammation.
(3) Curcumin is used to scavenge free radicals, anti-oxidation, activate NRF2, and reduce systemic chronic inflammation.
(4) Sulforaphane is used to scavenge free radicals, anti-oxidation, activate NRF2, and reduce systemic chronic inflammation.
(5) American ginseng is sliced for making tea or taken American ginseng capsules to replenish qi.
7.What Exercises Are Beneficial To Improving Long COVID Symptoms Of Loss Of Smell?
Taking the patient above as an example, we give the following exercise advice based on her condition:
(1) Olfactory recovery training. Generally, olfactory recovery training consists of three parts: odor essential oil, corresponding image card of cognitive recognition, and nasal wash. The common essential oils used are sweet orange essential oil, eucalyptus essential oil, rose essential oil, lemon essential oil, and clove essential oil. Recognition cards of cognitive image are images with text, and memory points corresponding to different essential oils, accompanied by olfactory conduction diagrams. Nasal wash can be usually performed with normal saline or normal saline supplemented with trace amounts of corticosteroids. Adherence to olfactory recovery training will achieve good results with twice a day, 1 minute each time for three months.
(2)Enjoy the wild of natural oxygen bars, such as walking in the deep forest, and perform deep breathing exercises.
(3) Assist nasal massage, eye exercises, and head massage.
8.What Is Beneficial To Improving Long COVID Symptoms Of Loss Of Smell In Terms Of Diet And Sleep?
Taking the patient above as an example, we give the following diet and sleep advice based on her condition:
(1) Eat more foods with rich or strong odors, such as onions, onions, garlic, and leeks, to stimulate both smell and taste.
(2) Drink half a cup of warm water before going to bed and after waking up to warm the nasal cavity. If the air is too dry, a humidifier can be used, but only to be added with pure water without other additives.
9.Patients With Loss Of Smell Or Olfactory Dysfunction Are Welcome To Contact With Our Long COVID Care Center
If there are similar symptoms among readers, contact our Long COVID Care Center for assistance.
Phone: +852 5765 5768
Whatsapp: +852 5765 5768
WeChat: longcovidcarecenter
Email: support@longcovidcarecenter.org
【Disclaimer: The treatment of diseases is a very complex and professional affair. Due to the limitation, Long COVID Care Center can only carry out remote simple interviews, unable to face-to-face offline interviews and obtain comprehensive physical examination results. Therefore, the suggestions, guidance, protocols, and documents conveyed by Long COVID Care Center to patients can only be used as a reference for patients to understand their diseases in many aspects, but cannot be directly used as a treatment plan. Patients must discuss their symptoms with doctors in local hospitals through face-to-face communication. After the patients completed the physical examination required by doctors, they would get a prescription issued by doctors and get the treatment under the guidance of doctors. Therefore, Long COVID Care Center hereby declares that our center is completely exempted from liability when any adverse consequences are caused by self-treatment of the patient for applying any contents convoyed by the center, that is, we do not bear any responsibilities.】

